Confused By the Latest Health Headlines? No Worries, We’ve Got Your Back!
2026 is barely two weeks old and already two big pieces of health news have disrupted the status quo. Both announcements were well-intentioned, a bit complicated, and a good reminder of why navigating healthcare without solid support has become harder than ever.
One came from the Federal government: updated dietary guidance that has people talking (and arguing a bit) about red meat, cheese, and what belongs on our plates. The other came from the FDA: approval of a new oral GLP-1 medication that has expanded a class of drugs already reshaping how we treat diabetes and obesity.
Let’s take them one at a time and then look at what they have in common.
Headline #1: The New US Dietary Guidelines
When Robert F. Kennedy Jr., Secretary of Health and Human Services, released the new dietary guidelines earlier this month, he suggested he had a bold new approach to “make America healthy again.” The new catch phrase is “Eat Real Food,” as opposed to the highly processed foods that help cause obesity, diabetes, and other diseases.

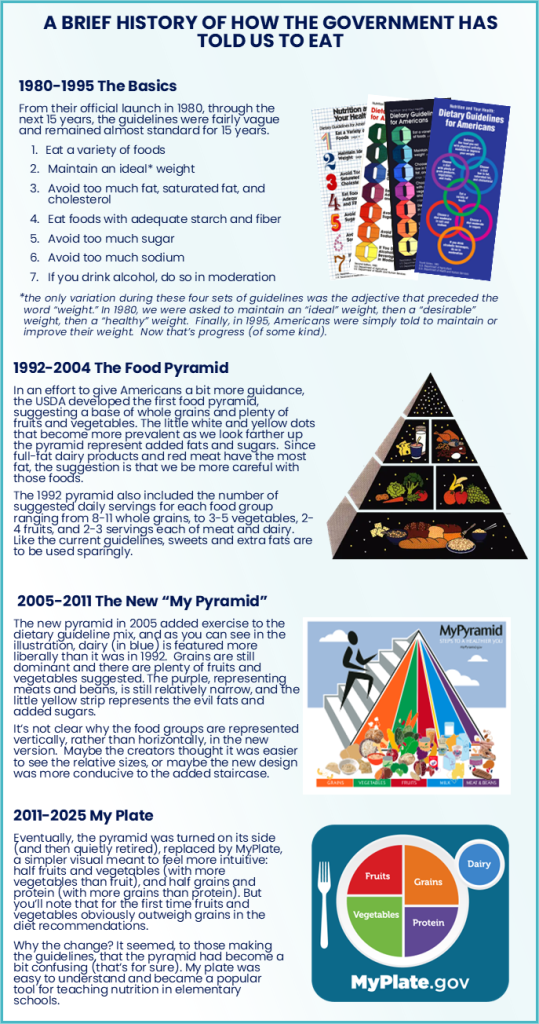
This is hardly a new concept. Since the first official US Dietary Guidelines (see timeline chart below), Americans have been warned against foods with added sugars. During the past decade, the dangers of “ultra-processed foods” (UPCs) have dominated dietary headlines. As a matter of fact, if you look at all the past food pyramids, only the first, in 1992, even suggested the consumption of added fats and sugars, with the little unlabeled triangle on top. And, there has never been a guideline or a pyramid that suggested we put ultra processed foods on our plates.
So, what is new about the new food pyramid? Well for one thing, it’s upside down, so it’s not so much a pyramid. According to RFK Jr., this pyramid is designed to “end the war on protein.” That’s a decades old war that hasn’t been raging lately since American consumers appear to be seeking protein now more than ever (see our recent protein email). What is different about the new pyramid is that it appears to promote more red meat and full-fat dairy than ever before. Whole grains are now relegated to the little triangle at the top (now bottom) of the pyramid where the least healthy foods traditionally live.
Why We Might Need Guidance on the New Guidelines
There is no question that swapping soda, pastries, and manufactured foods for whole foods is a superlative suggestion. And, for better or worse, many popular weight loss trends emphasize protein over carbohydrate-loaded grains. But again, those recommendations are not so new.
The placement of red meat and full-fat dairy in the “eat loads” section of the pyramid is what has raised some concern in the healthcare community. It is likely that those foods, which are notably high in saturated fat, have gotten better placement this year because we now know that saturated fat is not a direct cause of coronary artery disease, and that the inflammation caused by processed foods with added sugar is much more damaging to our cardiovascular health than saturated fat.
The reality is that most of us eat processed foods and may consume other things, like alcohol, that cause inflammation. And some of us have other risk factors for cardiovascular disease. In all those cases, eating red meat and full-fat dairy with abandon can cause problems. Prevailing research still shows that diets high in saturated fat, especially when combined with the choline also found in high-fat foods, can contribute to artery plaque and cardiovascular disease. That’s particularly relevant for people with existing heart disease, diabetes, or genetic risk factors. The latest research attributes that connection to an alteration of gut bacteria (yes, this may be too much information).
The point is: Less sugar? Good. More whole foods? Also, good. Unlimited steak and cheese? Definitely not for all of us. Only biometrics and a medical professional who knows your history can help you decide whether these recommendations are right for you.
Nutrition science evolves. But individual risk still matters more than broad guidance.
Headline #2: Wegovy in a Pill!
Last week’s approval of an oral version of Wegovy, the most commonly used GLP-1 receptor agonist for weight loss, immediately changed the weight loss landscape. GLP-1 receptor agonists aren’t new. These medications have been used for years to treat type 2 diabetes, and more recently, obesity. They work by slowing digestion, reducing appetite, improving insulin response, and helping regulate blood sugar.
Until now, they’ve largely been available as injections. The FDA’s approval of a once-daily oral Wegovy pill marks a shift, not because it changes how the drug works, but because it increases the number of people who may realistically use it.
Who might benefit from the pill instead of injections
The oral option may make sense for:
- People who qualify for GLP-1 therapy but are needle-averse
- Patients who prefer a daily pill routine
- Those who need tighter glucose control but aren’t seeking maximum weight loss
- People earlier in their treatment journey
Injectable GLP-1s may still be more effective for significant weight loss and certain metabolic goals. The pill isn’t “better,” it’s another tool, and the right choice depends on medical history, goals, side effects, cost, and coverage.
What’s coming next?
More GLP-1 options are already in development. A Zepbound pill is expected to be approved and on the market in just a few months. We’ll also see the development of combination therapies, longer-acting oral medications, drugs with fewer side effects, and treatments aimed at preserving muscle mass while reducing fat.
Off-brand GLP-1 receptor agonists are being sold in hundreds of online pharmacies. Prices of the brand names are dropping, and manufacturers are creating programs to sell directly to consumers. This space is moving fast, and headlines rarely capture the full picture. As many as 70% of Americans are overweight or obese and there are an increasing number of GLP-1 receptor agonists available. But how do any of us know which formula, dose, or delivery mechanism, if any, is right for us?
What Do These Two Developments Have in Common?
Dietary guidelines shift. Medications evolve. Headlines simplify.
But our bodies, our risks, and our goals don’t change every news cycle.